Sigarayı Bırakmada Nefes Egzersizleri: Araştırmalar Ne Diyor?
Sigarayı bırakmaya çalışırken o şiddetli istek (kriz) vurduğunda, genellikle "sadece derin bir nefes al" denir. Bu tavsiye, etkili olamayacak kadar basit bir klişe —gerçek bir stratejiden ziyade geçiştirme cümlesi— gibi duyulabilir. Ancak bu yönlendirme, göründüğünden çok daha sağlam bilimsel temellere dayanmaktadır. Kontrollü nefes egzersizleri, nikotinin beyninizde kullandığı sinir sistemi yollarını doğrudan etkiler. Klinik araştırmalar da belirli nefes tekniklerinin kriz yoğunluğunu, stresi ve yoksunluk belirtilerini ciddi oranda azaltabildiğini doğruluyor.
Tabii her nefes tekniği aynı düzeyde bilimsel kanıta sahip değil. Bazıları doğrudan sigara içicileri üzerinde yapılan klinik deneylerle test edilirken, bazıları genel stres yönetimi üzerinden bu sürece dahil ediliyor. Bu yazıda, teknikler arasındaki farkları net bir şekilde ortaya koyuyoruz. Nefesin nikotin isteğini nasıl bastırdığını bilimsel olarak inceleyecek ve size en uygun yöntemi seçebilmeniz için kanıtlanmış teknikleri "kanıt düzeyine göre" paylaşacağız. Böylece araştırmaların tam olarak neyi gösterip neyi göstermediğini bilerek ilerleyebilirsiniz.
⚡ Özetle: Şu An Bir Sigara Krizi Yaşıyorsanız
Eğer dikkatiniz şu anki şiddetli bir aşerme nedeniyle dağılmış durumdaysa, bilimsel açıklamaları atlayın ve hemen şunu uygulayın:
- Ritminizi bulun: Burnunuzdan 5 saniye boyunca yavaşça nefes alın.
- Yavaşça bırakın: Burnunuzdan veya dudaklarınızı büzerek 5 saniye boyunca nefes verin.
- 3 dakika boyunca tekrarlayın: Dakikada 6 nefeslik bu ritim "rezonans frekansı" olarak adlandırılır. Sinir sisteminizi "savaş ya da kaç" modundan çıkarıp "dinlen ve onar" moduna sokarak krizler için biyolojik bir durdurma düğmesi görevi görür.
Nikotin Krizi Nörobiyolojisi ve Nefesin Müdahale Gücü
Nefes egzersizlerinin krizleri nasıl azalttığını anlamak için önce krizlerin neden ortaya çıktığını bilmek gerekir. Nikotin, beyindeki reseptörlere bağlanarak mezolimbik ödül yolunda (beynin ana zevk ve alışkanlık merkezi) dopamin salınımını tetikler. Sürekli kullanımda beyin bu duruma uyum sağlar ve normal fonksiyonlarını sürdürmek için nikotine ihtiyaç duyar. Sigara kesildiğinde sistem açık verir; bu da huzursuzluk, sinirlilik, konsantrasyon bozukluğu ve şiddetli sigara içme arzusu olarak kendini gösterir.
Bu süreçte stres tepki sistemi de devreye girer. Nikotin yoksunluğu, sempatik sinir sistemi aktivitesini (savaş ya da kaç tepkisi) artırır; bu da kortizol salınımını ve kalp atış hızını yükseltirken kalp atış hızı değişkenliğini (HRV) düşürür. Düşük HRV, vücudunuzun gevşeme yeteneğinin azaldığını gösterir ve kriz yoğunluğu ile nüks etme olasılığıyla doğrudan ilişkilidir.
Kontrollü nefes egzersizleri tam da bu noktada devreye girer. Dakikada yaklaşık 5-6 döngü olacak şekilde yapılan yavaş diyafram nefesi, vagus siniri yoluyla beyne sakinleştirici mesajlar gönderir. Bu durumun ölçülebilir sonuçları vardır: HRV artar, kortizol seviyeleri düşer ve beynin krizle ilişkili bölgelerindeki (insula, amigdala) aktivite dengelenir. Little ve ark. (2025) tarafından yayınlanan güncel bir inceleme, yavaş ve burundan yapılan diyafram nefesinin tam da nikotin yoksunluğuyla bozulan fizyolojik profili düzelttiğini doğrulamıştır.
Otonom Değişimi Görselleştirmek
Kontrollü nefes, sinir sisteminiz için bir "manuel müdahale" işlevi görür. Nefesinizin ritmini değiştirerek vücudunuzu yüksek alarm durumundan çıkarıp iyileşme moduna sokabilirsiniz.
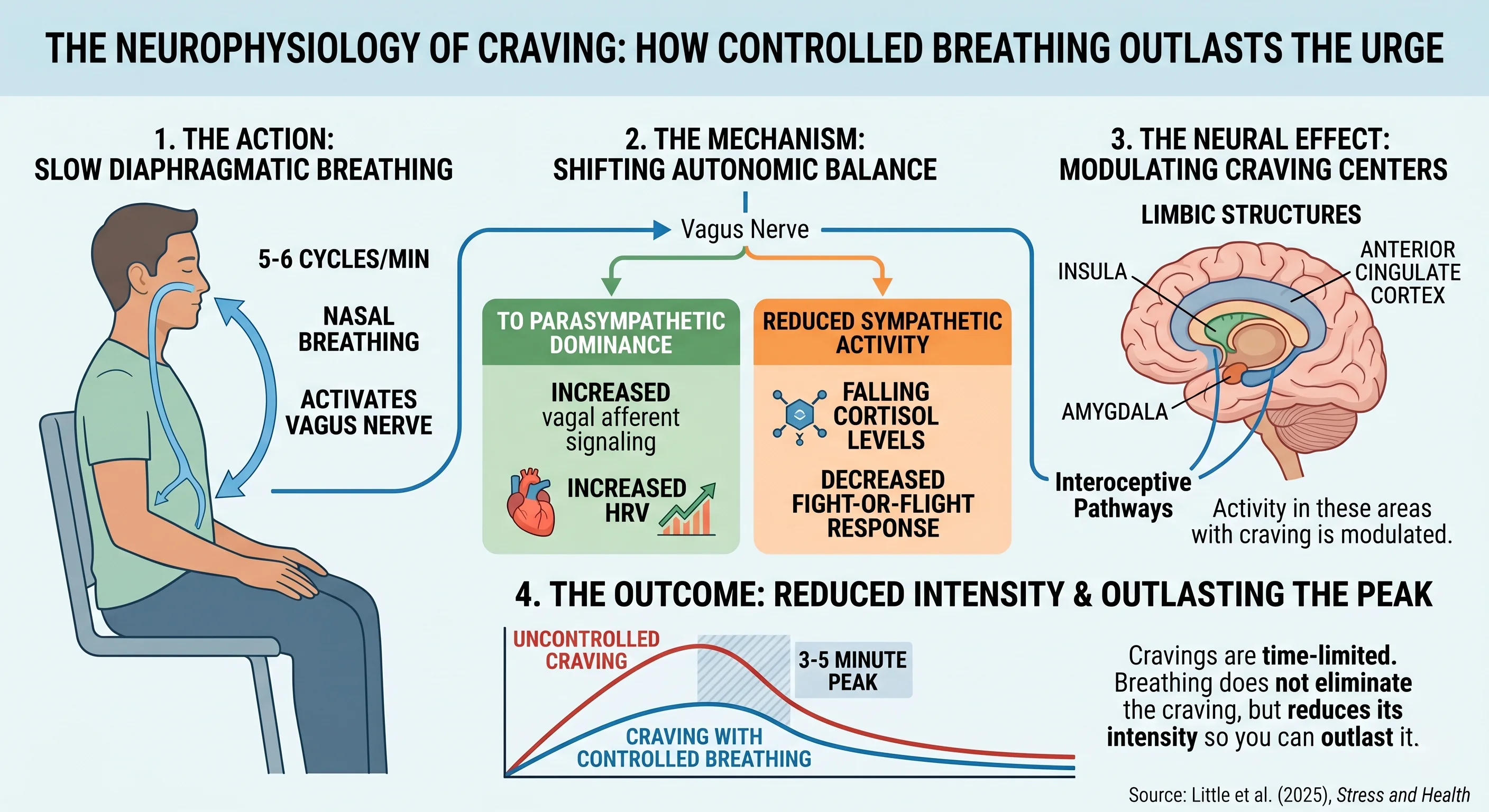
Nöral düzeyde bir kriz, süresi sınırlı bir olaydır. Araştırmalar, krizlerin yaklaşık 3 ila 5 dakikada zirveye ulaştığını ve kişi sigara içse de içmese de yatıştığını gösteriyor. Nefes egzersizlerinin amacı krizi tamamen yok etmek değil; yoğunluğunu, kişinin bu süreyi atlatabileceği seviyeye indirmektir.
Klinik Kanıtlar: Araştırmalar Ne Diyor?
Sigara bırakma ve nefes egzersizleri üzerine yapılan klinik çalışmalar, artık anlamlı sonuçlar çıkarmamıza yetecek düzeydedir.
Nefes ve kriz üzerine yapılan ilk kontrollü araştırmalardan biri (McClernon ve ark., 2004), her 30 dakikada bir alınan 5 derin nefesin, sigara içicilerinde kriz oranlarını ve negatif duyguları kontrol grubuna göre önemli ölçüde düşürdüğünü saptamıştır.
En çarpıcı kanıtlardan biri ise Price ve ark. (2022) tarafından yapılan randomize klinik deneydir. Araştırmada, rezonans nefesi (dakikada 6 nefes) uygulayan kadın bağımlıların, kriz anlarında kontrol grubunda görülen "kriz tırmanışını" engellediği görülmüştür. Bu, genel bir gevşemeden farklı olarak, kriz tepkisine o anda doğrudan müdahale edildiğini kanıtlamaktadır.
Shahab ve ark. (2013) tarafından 96 katılımcı ile yapılan bir deneyde, diyafram ve burun deliklerini değiştirerek yapılan 10 dakikalık nefes pratiğinin kriz ölçümlerini anında ve ciddi oranda azalttığı tespit edilmiştir.
En güncel verilerden biri olan Kumar ve ark. (2026) çalışması ise, yüksek bağımlılığa sahip içicilerde 4 haftalık düzenli nefes pratiğinin ardından kriz sıklığının %38,5, yoğunluğunun ise %39,4 azaldığını göstermiştir. Ayrıca katılımcıların akciğer fonksiyonlarında (FEV₁) %17,98'lik bir iyileşme kaydedilmiştir.
Kriz Yönetimi İçin Kanıt Destekli Nefes Teknikleri
Aşağıdaki teknikler, sigara bırakma ve kriz yönetimi üzerindeki kanıt düzeylerine göre sıralanmıştır. İlk iki teknik doğrudan sigara içicileri üzerinde test edilmiştir.
1. Rezonans / Tempolu Nefes (Dakikada 6 Nefes)
En iyi kanıt: Kriz anlarında krizin tırmanmasını engelleme
Bu teknik, dakikada tam olarak 5 ila 6 tam döngü (yaklaşık 5 saniye nefes al, 5 saniye nefes ver) yapılmasını içerir. Bu ritim, kan basıncının doğal dalgalanmasıyla (Mayer dalgaları) uyum sağlar ve vücudun üretebileceği en güçlü parasempatik (sakinleştirici) tepkiyi oluşturur (Lehrer & Gevirtz, 2014).
Price ve ark. (2022) çalışması, bu spesifik hızın krizleri bloke ettiğini göstermiştir. Normal nefes hızı (dakikada 14 nefes) aynı etkiyi yaratmamaktadır; kriz yönetimindeki farkı yaratan bu spesifik yavaşlıktır.
Nasıl Uygulanır: Dik bir omurga ile rahatça oturun. Burnunuzdan 5 saniye boyunca, karnınızın yükselmesine izin vererek (diyaframı kullanarak) yavaşça nefes alın. Yine burnunuzdan 5 saniye boyunca yavaşça verin. Nefes alıp verme arasında duraksamadan akıcı bir ritim yakalayın. Dikkatin dağıldığı kriz anlarında bir metronom veya görsel bir rehber kullanmak çok faydalıdır.
2. Diyafram (Karın) Nefesi
En iyi kanıt: Anlık kriz azaltma ve negatif duyguların giderilmesi
Diyafram nefesi, diğer tüm tekniklerin temelidir ve sigara içicileri üzerinde en geniş kanıt tabanına sahip yöntemdir. Stres anında kullanılan omuz ve göğüs nefesi yerine, ana solunum kası olan diyaframın aktif kullanılmasını hedefler.

McClernon (2004), Shahab (2013) ve Kumar (2026) gibi temel tüm çalışmalar bu tekniğin kriz yoğunluğunu anında azalttığını doğrulamaktadır.
Nasıl Uygulanır: Bir elinizi göğsünüze, diğerini karnınıza koyun. Burnunuzdan 4-5 saniye boyunca nefes alın; göğsünüz sabit kalırken sadece karnınızın şiştiğinden emin olun. Ardından 5-6 saniye boyunca yavaşça nefes verin.
👉 Şimdi Dene: İnteraktif Diyafram Nefesi Aracı
3. Alternatif Burun Nefesi (Nadi Shodhana)
En iyi kanıt: Düzenli günlük pratikle kriz sıklığını azaltma
Bu teknikte burun delikleri sırayla kapatılarak nefes alınır. Shahab (2013) ve Kumar (2026) çalışmalarında bu yöntemin 10 dakikalık uygulamalarda kriz ölçümlerini ciddi şekilde düşürdüğü görülmüştür.
Nasıl Uygulanır: Sağ burun deliğini kapatıp soldan 4-5 saniye nefes alın. Her iki deliği kısa süre kapalı tutun. Sağdan 5-6 saniye boyunca nefes verin. Sonra sağdan alıp soldan vererek döngüyü tamamlayın.
Daha çok sabah rutinleri gibi planlı zamanlarda yapılması önerilir; kriz anında anlık bir tepki olarak uygulanması diğerlerine göre daha zordur.
4. Kutu Nefesi (4-4-4-4)
En iyi kanıt: Yoksunluk sırasında zihinsel netlik ve stres yönetimi
Askeri personel ve acil durum ekipleri tarafından yoğun stres altında kullanılan bu yöntem (4 saniye al, 4 saniye tut, 4 saniye ver, 4 saniye tut), zihinsel netlik sağlar. Sigara bırakma özelinde doğrudan bir klinik deneyi olmasa da, genel stres yönetimi kanıtları nedeniyle bırakma sürecindeki "zihin bulanıklığı" için önerilir.
Nasıl Uygulanır: 4 saniye nefes al, 4 saniye nazikçe tut, 4 saniye ver, 4 saniye tut. Ritmi korumak kolay olduğu için çalışma ortamlarında tercih edilebilir.
👉 Şimdi Dene: İnteraktif Kutu Nefesi Aracı
5. 4-7-8 Tekniği
En iyi kanıt: Şiddetli kaygıyı azaltma ve gevşeme
Dr. Andrew Weil tarafından popülerleştirilen bu yöntemde 4 saniye nefes alınır, 7 saniye tutulur ve 8 saniye boyunca (vısh sesi çıkararak) verilir. Uzun süreli nefes verme, sakinleştirici sinir sistemini en güçlü şekilde aktive eden mekanizmadır.
Vierra ve ark. (2022), 3 setlik 4-7-8 nefesinin kalp atış hızını ve kan basıncını anında düşürdüğünü kanıtlamıştır. Bu teknik, sigara içicilerinde doğrudan test edilmese de, vücutta yarattığı fizyolojik değişim bırakma sürecindeki ihtiyacı tam olarak karşılar.
👉 Şimdi Dene: İnteraktif 4-7-8 Nefes Aracı
Kapsamlı Bir Stratejinin Parçası Olarak Nefes
Araştırmalar, nefes egzersizlerini ilaç veya davranışçı terapi gibi yöntemlerin yerine değil, onları destekleyen bir güç çarpanı olarak görmeyi öneriyor. Nefes egzersizleri ücretsizdir, yan etkisi yoktur ve krizin vurduğu o kritik saniyelerde anında uygulanabilir. Kriz geçici bir durumdur; nefes egzersizleri ise o geçiş süresini katlanılabilir kılan en etkili araçtır.
Pratik Uygulama Planı
Sigarayı bırakmaya yeni başlayanlar için literatürdeki verilere dayanan önerimiz şudur:
- İlk Hafta: Krizlerin en yoğun olduğu dönemde, ilk belirtiyi hissettiğiniz an diyafram nefesine başlayın ve 3-5 dakika sürdürün.
- Günlük Pratik: Krizler daha gelmeden sinir sisteminizi güçlendirmek için her sabah 5-10 dakika rezonans nefesi (5 al, 5 ver) çalışın. Bu, krizlerin genel şiddetini 2-4 hafta içinde düşürecektir.
Önemli Çıkarımlar
Nefes egzersizleri, vagus siniri uyarımı ve HRV artışı gibi net fizyolojik yollarla nikotin isteğini azaltır. Bilimsel kanıtlar, kriz tırmanışını engellemek için dakikada 6 nefeslik rezonans ritmini ve genel kriz yönetimi için diyafram nefesini ön plana çıkarmaktadır. Düzenli kullanıldığında bu egzersizler, sigarayı bırakanlar için en erişilebilir ve etkili araçlardan biridir.
Quitbook Nasıl Destekler?
Quitbook, klinik literatürde tanımlanan 3-5 dakikalık kriz pencerelerine özel olarak tasarlanmış, rezonans hızında tempo tutan rehberli nefes egzersizleri içerir.

Uygulama, tetikleyicileri incelemek için BDT tabanlı düşünce günlüğü ve kişiselleştirilmiş hedeflerle birleşerek, bırakma sürecinin hem fiziksel hem de psikolojik boyutlarını tek bir noktada çözer.
Quitbook yakında sizlerle. Bekleme listesine katılın.
Kaynaklar
- McClernon, F.J., et al. (2004). The effects of controlled deep breathing on smoking withdrawal symptoms. Addictive Behaviors.
- Shahab, L., et al. (2013). The acute effects of yogic breathing exercises on craving. Psychopharmacology.
- Price, J.L., et al. (2022). Effects of resonance breathing on craving in women with substance use disorder. Addictive Behaviors.
- Kumar, S., et al. (2026). Volitional yoga breathing for smokers: pulmonary rehabilitation and craving management. Cureus.
- Lehrer PM, Gevirtz R. (2014). Heart rate variability biofeedback: how and why does it work? Front Psychol.
- Vierra, J., et al. (2022). Effects of 4-7-8 breathing control on heart rate variability. Physiological Reports.
- Priasmoro, D. P., et al. (2025). Exploring 4-7-8 breathing for stress relief: a scoping review. ICISTECH.
- Little, H., et al. (2025). The A52 Breath Method: a narrative review of breathwork for mental health. Stress and Health.
Tıbbi Uyarı: Bu makale bilgilendirme amaçlıdır ve tıbbi tavsiye niteliği taşımaz. Herhangi bir programa başlamadan önce mutlaka bir sağlık uzmanına danışın.
Bu makalede bahsedilen teknik
QuitBook Mobil Uygulaması
İlerlemeni takip et, krizleri yönet ve ne kadar tasarruf ettiğini hesapla.
Google Play'den İndirSıradaki Okuma
Sigarayı Bırakmanın Sağlık Faydaları: Hafta Hafta İyileşme Zaman Çizelgesi
20 dakikadan 15 yıla: Sigarayı bıraktığınızda vücudunuzda neler olduğunun klinik temelli, adım adım haritası — ve en zor haftanın neden en büyük kazanımları getirdiği.
Nikotin Yoksunluğu: Belirtiler, Zaman Çizelgesi ve Neler Bekleyeceğiniz
Nikotin yoksunluğunun klinik temelli, haftalık haritası — her belirtinin ne olduğu, nörolojik açıdan neden yaşandığı ve o an için kanıta dayalı olarak yapılması gerekenler.