Wired Differently, Hooked Harder: The Neuroscience of Smoking in ADHD
If you have tried to quit smoking more than once — and watched yourself relapse not from lack of effort but from a strange cognitive unravelling, a fog that settles in and makes sustained intention feel impossible — there is a possibility that your cessation attempts have been treating the wrong problem.

A substantial and growing body of research makes this uncomfortable: people with Attention Deficit Hyperactivity Disorder (ADHD) are approximately two to three times more likely to smoke than the general population, start smoking earlier, smoke more cigarettes per day, experience more severe withdrawal symptoms, and have significantly lower quit rates. Among adult smokers, prevalence rates for ADHD run as high as 40%, compared to roughly 20% in the general population. Among those who do attempt to quit, only 29% of smokers with ADHD achieve abstinence compared to 48.5% of smokers without the condition.
These are not marginal differences. They suggest that a large proportion of people who feel like they have "failed" at quitting may be contending with neurobiological factors that standard cessation advice — built around the assumption of intact executive function — was never designed to address.
This article does not argue that ADHD explains all smoking or all relapse. What it does argue, based on the clinical literature, is that the relationship between ADHD and nicotine is mechanistically specific, that this mechanism makes quitting genuinely harder in ways that are not fully captured by terms like "low willpower" or "high addiction," and that cessation approaches which account for the ADHD brain produce meaningfully better outcomes than those that do not.
A person trying to quit smoking with unrecognised ADHD is not weak-willed. They are fighting with one hand tied behind their back, against a disadvantage they have no language for.
— QuitBook · Neuroscience & Behaviour
The ADHD Brain: A Dopamine Deficit That Predates the First Cigarette
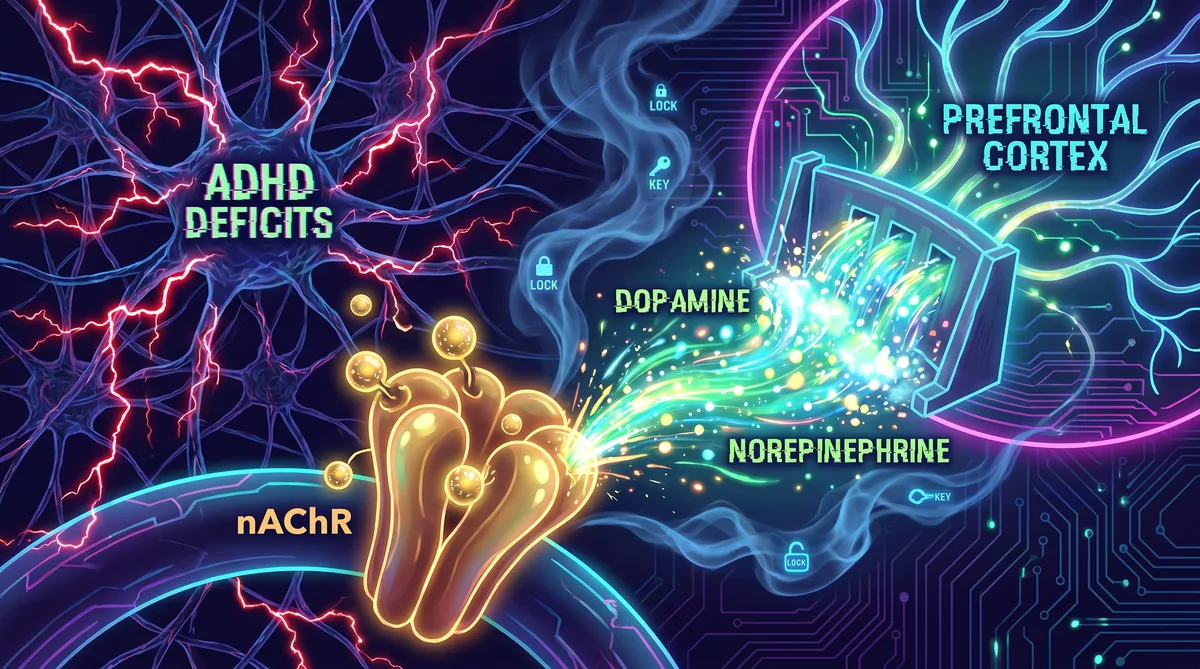
ADHD is commonly described as an attention disorder, but this framing obscures its neurobiological core. At the level of brain function, ADHD is primarily characterised by dysregulation of the dopamine and norepinephrine systems, particularly in the circuits connecting the prefrontal cortex (PFC) to the striatum and limbic structures.
The prefrontal cortex is the brain's executive hub. It governs working memory — the ability to hold information in mind while using it — inhibitory control, planning, attention regulation, and emotional modulation. In ADHD, PFC function is compromised not because the structure is damaged but because it is chronically underfuelled. Dopamine and norepinephrine signalling in these circuits is weaker than in neurotypical brains, and the result is a cluster of functional deficits: difficulty sustaining attention on low-stimulation tasks, impaired ability to suppress prepotent impulses, reduced working memory capacity, and emotional dysregulation that can look, from the outside, like volatility or poor motivation.
One of the most clinically important features of the ADHD brain is an altered response to reward and time. Research consistently shows that individuals with ADHD discount delayed rewards at a steeper rate than controls — a phenomenon known as delay discounting. When the choice is between a small immediate reward and a larger future reward, the ADHD brain weights the immediate option more heavily, not as a character failing but as a product of dysregulated dopamine signalling in the striatum. This is directly relevant to cessation: quitting smoking is a paradigmatic delay discounting challenge, requiring the sustained sacrifice of an immediate dopamine hit for long-term health that will not manifest for months or years.
This neurobiological profile creates a compounding vulnerability to nicotine specifically. Before the first cigarette is ever smoked, the ADHD brain is already characterised by the precise dopaminergic deficits that nicotine is exceptionally well-suited to temporarily correct.
Nicotine as a Cognitive Prosthetic
The self-medication hypothesis of smoking in ADHD is not a folk theory. It has substantial mechanistic and clinical support, and it explains a pattern that clinicians working with ADHD populations frequently observe: smoking often begins not at parties or through peer pressure alone, but during periods of cognitive demand — studying, working, managing emotionally complex situations — and its perceived effects are not primarily relaxation but focus, clarity, and emotional steadiness.
Nicotine's mechanism in the brain begins at the nicotinic acetylcholine receptors (nAChRs), particularly the α4β2 subtype that is heavily expressed in the prefrontal cortex and striatum. When nicotine binds to these receptors, it triggers the release of dopamine, norepinephrine, acetylcholine, and glutamate in a pattern that directly addresses the neurotransmitter deficits characteristic of ADHD. Dopamine release in the PFC and nucleus accumbens improves signal-to-noise ratios in working memory circuits. Norepinephrine enhancement in the PFC sharpens attention and inhibitory control. The acute cognitive effect of nicotine on the ADHD brain is not imagined — it is pharmacologically real.
Laboratory studies have confirmed this. Research has shown that nicotine improves working memory, sustained attention, and behavioural inhibition in individuals with ADHD, and that these improvements are more pronounced in ADHD populations than in controls. In some studies, acute nicotine administration has produced cognitive improvements in ADHD individuals comparable in magnitude to low-dose stimulant medications. This is the mechanism behind a pattern that many ADHD smokers recognise but rarely have words for: the cigarette is not just pleasurable; it feels cognitively necessary.
More recently, research has complicated this picture in an important way. Tobacco smoke contains not only nicotine but also monoamine oxidase inhibitors (MAOIs), compounds that slow the breakdown of dopamine and other monoamines in the brain. A 2022 scoping review in Frontiers in Neuroscience found evidence that the MAOI activity in tobacco smoke may contribute to dopamine availability beyond what nicotine alone provides — meaning that nicotine replacement therapies, which deliver nicotine without the MAOI component, may be failing ADHD smokers partly because they replace only one part of the neurochemical relief that smoking was providing.
The cruel precision of this mechanism is worth sitting with. A person with ADHD who begins smoking in adolescence may be doing so before they have ever received a diagnosis, before they have any language for why they feel perpetually behind, why tasks that seem straightforward for others require enormous effort from them, why their emotions run hotter. Nicotine provides a real, if temporary and harmful, solution to a real neurobiological problem. And when they try to quit, they are not just withdrawing from a drug. They are losing the cognitive scaffolding they built around it.
Why Standard Cessation Advice Fails This Population
Standard smoking cessation approaches rest on several implicit assumptions: that the person can form and hold a clear intention to quit, that they can track and respond to triggers consistently over time, that they have sufficient working memory to execute multi-step coping plans in the moment a craving strikes, and that the primary challenge of quitting is managing the urge to smoke rather than managing a cognitive deterioration that follows from not smoking.
For people with ADHD, each of these assumptions is undermined.
Withdrawal is cognitively worse. Research using delay discounting tasks has found that smoking abstinence significantly increases impulsive behaviour in people with high ADHD symptoms — a pattern not seen to the same degree in low-symptom smokers. When a person with ADHD stops smoking, the dopamine deficit that characterised their brain before the first cigarette returns, but now the brain has adapted to higher baseline nicotine levels. Withdrawal does not just produce physical craving; it produces a measurable decline in inhibitory control and a steeper discounting of future rewards. The cognitive state that makes quitting feel impossible is, in part, a genuine neurobiological consequence of abstinence.
Standard NRT replaces the addiction but not the function. Nicotine replacement therapy is effective for many smokers because it manages the physical withdrawal while behavioural changes are made. For ADHD smokers, the calculation is different. NRT provides nicotine without the MAOI component of smoke and without the rapid dopamine spike produced by inhaled nicotine — and that spike, however harmful, was providing real cognitive relief. Many ADHD smokers who attempt NRT report that they continue to experience cognitive fog, concentration failure, and emotional dysregulation at levels that make sustained cessation extremely difficult.
Standard CBT assumes stable executive function. Cognitive behavioural therapy for smoking cessation works by helping people identify triggers, plan coping responses, and restructure thoughts about smoking. This requires working memory to recall coping plans, inhibitory control to suppress the impulse while the plan is executed, and sustained attention to notice and respond to triggers before they become fully formed cravings. All three of these capacities are impaired in ADHD — and more impaired during withdrawal. A person with ADHD following a standard CBT cessation program is being asked to apply executive function tools at the moment their executive function is most compromised.
Inattentive symptoms predict poorer cessation outcomes independently of treatment type. A secondary analysis of a randomised controlled trial of varenicline in adolescent and young adult smokers, published in 2023, found that participants with high inattentive ADHD symptoms at baseline were significantly less likely to achieve abstinence during treatment — and this pattern was not modified by whether they received varenicline or placebo (Green et al., 2023). The finding is important: it means that even one of the most effective cessation pharmacotherapies available does not fully compensate for the cessation disadvantage created by ADHD inattentive symptoms.
The diagnosis gap makes everything worse. An unknown but substantial proportion of adults with ADHD have never been diagnosed. Estimates suggest that roughly 75% of adults meeting criteria for ADHD do not carry a formal diagnosis. This means that for many people who have cycled through multiple failed quit attempts, no clinician has ever connected the dots between their cessation failures and their underlying neurobiology. They receive the same tools that work for neurotypical smokers, they fail at rates that reflect their neurobiological disadvantage, and they accumulate a history of "failed" quit attempts that functions as evidence of personal inadequacy rather than as a signal that the wrong framework is being applied.
What Actually Helps: Evidence-Based Approaches for ADHD Smokers
The news is not uniformly pessimistic. Research on cessation approaches adapted to the ADHD brain is still relatively thin compared to the general cessation literature, but several strategies have meaningful support.
Treat ADHD and smoking together, not sequentially. The most consistent finding in the literature is that treating ADHD with stimulant medication — which directly addresses the dopamine deficit — reduces smoking rates in ADHD populations. A meta-analysis by Schoenfelder et al. found that long-term stimulant treatment was associated with significant reductions in smoking behaviour, challenging earlier concerns that stimulants might increase addiction risk. For adults in cessation who have undiagnosed or undertreated ADHD, achieving adequate ADHD symptom control may be as important as any cessation-specific intervention. If you have tried to quit multiple times and relapsed in the context of what felt like cognitive collapse rather than simple craving, raising the possibility of ADHD assessment with your GP or psychiatrist is clinically warranted.
Extended and higher-dose NRT. Standard NRT programs run 8 to 12 weeks. For ADHD smokers, this is likely insufficient. The neurobiological adaptation to nicotine in ADHD populations is more entrenched, and the cognitive consequences of rapid nicotine reduction are more severe. Some clinicians and researchers advocate for extended NRT protocols — 24 weeks or longer — and higher initial patch doses for heavy smokers with ADHD symptoms. This is an area where the evidence base is still developing, but the mechanistic rationale is solid.
Varenicline remains the strongest pharmacological option, with caveats. Varenicline works by partially agonising the α4β2 nAChR — the same receptor subtype that nicotine uses — which reduces both craving and the rewarding effect of smoking. A study by Bidwell et al. (2017) found that among adult smokers with hyperactive-impulsive ADHD symptoms, varenicline was associated with fewer cigarettes per day and reduced withdrawal severity. The effect was not seen for inattentive symptoms in the same way, and varenicline alone does not equalise cessation outcomes for ADHD populations. It is best understood as a useful tool within a broader strategy rather than a standalone solution.
CBT adapted for ADHD. The adaptations required are straightforward but meaningful. Sessions that are shorter and more structured reduce the working memory demands of absorbing cessation information. Written and visual coping prompts — a card in the wallet, a note on the phone lock screen — externalise the coping plan so it does not have to be retrieved from working memory under craving pressure. Trigger identification benefits from immediate recording (a voice note immediately after a craving) rather than retrospective recall hours later, which ADHD working memory will not reliably support.
Mindfulness and ACT. Acceptance and Commitment Therapy, which forms one of the theoretical foundations of QuitBook, has specific applicability to ADHD cessation. ACT does not require the smoker to execute a complex coping plan; it requires them to notice a craving, accept its presence without reacting, and allow it to pass. This is a more attainable in-the-moment cognitive task than multi-step CBT coping chains, and ACT-based interventions have shown efficacy in both ADHD and cessation contexts independently.

Breathing exercises: a direct neurobiological fit. Slow, controlled breathing techniques have particular relevance for the ADHD cessation population for reasons that go beyond general craving management. The mechanisms are directly applicable. Diaphragmatic breathing at approximately six cycles per minute activates vagal afferent pathways, increases parasympathetic tone, and modulates activity in the prefrontal cortex and anterior cingulate — the same circuits that are dysregulated in ADHD. In the context of withdrawal, when PFC function is already impaired, breathing exercises provide a body-based regulation tool that does not require intact executive function to initiate. Inhale. Exhale. The instruction is simple enough to execute when the working memory is clouded and the impulse to smoke is loud.
The 4-7-8 technique, which produces a strong parasympathetic response through its extended exhalation, and resonance breathing at six cycles per minute, which blocks craving escalation through baroreflex activation, are both accessible during the acute withdrawal window. For the ADHD smoker who cannot hold a multi-step coping plan in mind while craving, a three-minute breathing exercise is a meaningful alternative that works through physiology rather than cognition.
A Public Health Gap Worth Naming
There is a pattern that runs through the literature on ADHD and smoking cessation that is worth naming plainly. Most cessation programs were designed without ADHD in mind. Most of the research on cessation outcomes does not screen for or stratify by ADHD status. Most people who cycle through multiple failed quit attempts are not asked whether they have ever been assessed for ADHD.
The consequence is that a population for whom quitting is neurobiologically harder receives the same support as everyone else, fails at higher rates, and typically attributes that failure to themselves. The framing of "failed quit attempt" becomes a moral accounting rather than a diagnostic signal.
If you have made serious quit attempts — not casual ones, but sustained efforts with commitment — and relapsed not from indifference but from a kind of cognitive and emotional disintegration that felt qualitatively different from simple craving, that pattern is worth discussing with a clinician. Not because ADHD is the only explanation, and not because a diagnosis changes everything overnight, but because treating the smoking while leaving the underlying neurobiology unaddressed means working against a disadvantage that does not have to be permanent.
The quit rate for smokers with well-managed ADHD who receive adapted cessation support is not the same as the quit rate for smokers with untreated, unrecognised ADHD trying to use programs designed for different brains. That gap represents a genuinely modifiable outcome.
Key Takeaways
People with ADHD smoke at roughly double the rate of the general population and quit at roughly half the rate, not because of weak motivation but because of specific neurobiological factors that standard cessation approaches do not address. Nicotine provides genuine, pharmacologically real cognitive relief for the dopamine deficits that characterise the ADHD brain — making smoking a form of self-medication that often predates any diagnosis. Standard NRT replaces the chemical without replacing the cognitive function; standard CBT assumes executive capacities that are impaired by the disorder itself and further impaired by withdrawal. Effective cessation for ADHD populations is most likely when ADHD is treated directly alongside the smoking, when NRT protocols are extended beyond standard durations, when coping tools are externalised rather than memory-dependent, and when body-based regulation techniques — including controlled breathing — are used to manage the acute cognitive and emotional disruption of withdrawal without requiring the executive resources that are simultaneously most needed and most depleted.
If you have relapsed repeatedly and the experience felt less like giving in to temptation and more like losing the ability to think clearly, that is a meaningful clinical distinction. It deserves a different question, not a repeated application of the same answer.
How QuitBook Supports This
QuitBook's tools are designed around the real-time craving window and the cognitive reality of withdrawal. The guided breathing exercises — calibrated to the three-to-five minute craving duration and paced to the resonance frequency — provide a body-based intervention that does not require intact working memory to initiate or maintain. The CBT-based thought journal creates an external record of triggers and responses that compensates for the retrospective recall failures common during withdrawal. For users who may be contending with ADHD symptoms — diagnosed or not — these tools address the craving experience at the physiological level, where regulation is still accessible when the cognitive level is overwhelmed.
Full References +
- Kollins, S.H., McClernon, F.J., & Fuemmeler, B.F. (2005). Association between smoking and ADHD symptoms. Archives of General Psychiatry, 62(10), 1142–1147.
- Humfleet, G.L., et al. (2005). History of childhood ADHD and smoking treatment failure. Nicotine & Tobacco Research, 7(3), 453–460.
- van Amsterdam, J., et al. (2018). Causal factors of increased smoking in ADHD. Substance Use & Misuse, 53(3), 432–445.
- Bidwell, L.C., et al. (2017). ADHD symptoms impact smoking outcomes in response to varenicline. Drug and Alcohol Dependence, 179, 18–24.
- Green, A., et al. (2023). ADHD symptoms and smoking outcomes in a RCT of varenicline. Drug and Alcohol Dependence, 244, 109774.
- McClernon, F.J., & Kollins, S.H. (2008). ADHD and smoking: from genes to brain to behaviour. Annals of the New York Academy of Sciences, 1141, 131–147.
- Gehricke, J.G., et al. (2007). Smoking to self-medicate attentional and emotional dysfunctions. Nicotine & Tobacco Research, 9(Suppl 4), S523–S536.
- Moen, O.A., et al. (2022). Tobacco and ADHD: a role of MAO-inhibition in nicotine dependence. Frontiers in Neuroscience, 16, 845646.
- Ashare, R.L., et al. (2011). Effects of smoking abstinence on impulsive behaviour in ADHD-like smokers. Psychopharmacology, 219(2), 537–547.
- Levin, E.D., et al. (2001). Effects of nicotine on cognitive function in ADHD. Psychopharmacology, 154(3), 257–267.
- Schoenfelder, E.N., et al. (2014). Stimulant treatment of ADHD and cigarette smoking: a meta-analysis. Pediatrics, 133(6), 1070–1080.
- Heishman, S.J., et al. (2010). Meta-analysis of the acute effects of nicotine on human performance. Psychopharmacology, 210(4), 453–469.
- McCabe, S.E., et al. (2025). JAMA Network Open.
Medical disclaimer: This article is for informational purposes only and does not constitute medical advice. If you suspect you may have ADHD and are seeking to quit smoking, please consult a qualified healthcare provider. Effective support is available, and a formal assessment can meaningfully change the options open to you.
QuitBook Mobile App
Track your progress, manage urges, and calculate your wealth saved.
Get it on Google PlayRead Next
The Health Benefits of Quitting Smoking: A Week-by-Week Recovery Timeline
From 20 minutes to 15 years: a clinically grounded, milestone-by-milestone map of what happens to your body when you quit smoking — and why the hardest week delivers the biggest gains.
What Is CBT for Smoking Cessation — and Does It Work?
Cognitive Behavioral Therapy is the most evidence-backed psychological approach to quitting smoking. Here is the science behind why it works — and how to apply it.